The PBT Study Group is chaired by Professor Christopher Nutting. The Study Group’s Deputy Chair is Dr David Thomson.
The NCRI CTRad National Proton Beam Radiotherapy Fellow Dr Romélie Rieu can be contacted via romelie.rieu@nhs.net.
As per the Research support tab, CTRad organises proposals guidance meetings to provide pre-submission peer input for UK radiotherapy studies in all stages of development, including for proton beam therapy proposals.
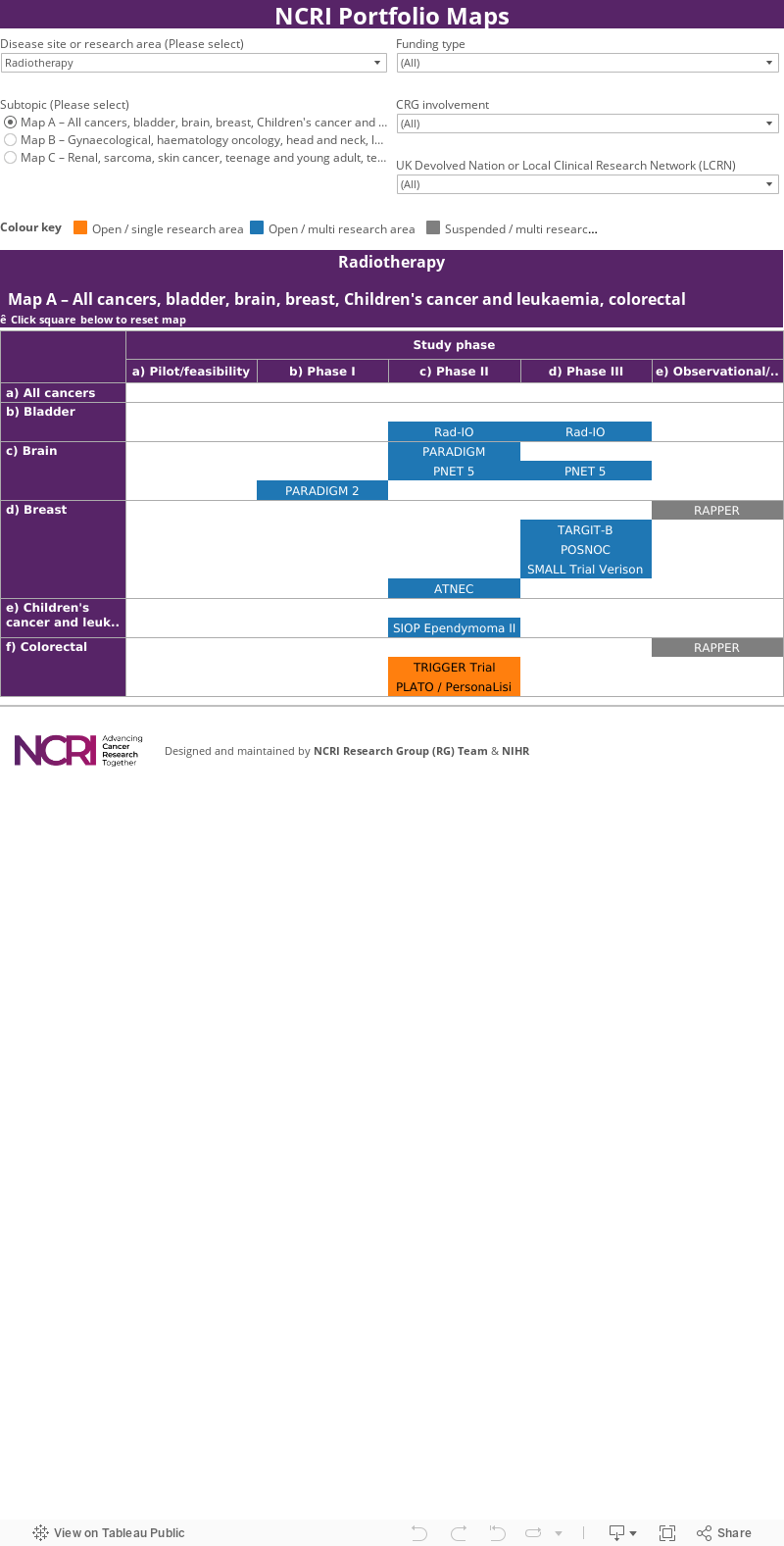
Below is summary information on PBT trials that are either recruiting or due to open quite soon (page last updated July 2023).